Ureteric Stone
Urinary Tract Stones (Urolithiasis)/ Ureteric Stone/ Renal calculi

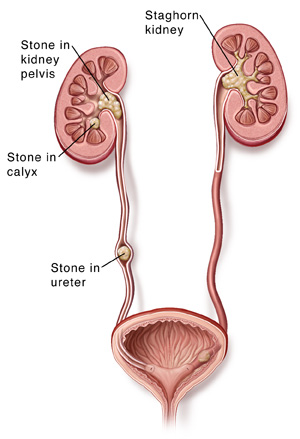
Ureteric colic is an important and frequent emergency in medical practice. It is most commonly caused by the obstruction of the urinary tract by calculi. Between 5–12% of the population will have a urinary tract stone during their lifetime, and recurrence rates approach 50%. Renal calculi are formed when the urine is supersaturated with salt and minerals such as calcium oxalate, struvite (ammonium magnesium phosphate), uric acid and cystine. 60-80% of stones contain calcium. They vary considerably in size from small ‘gravel-like’ stones to large staghorn calculi. The calculi may stay in the position in which they are formed, or migrate down the urinary tract, producing symptoms along the way. Studies suggest that the initial factor involved in the formation of a stone may be the presence of nanobacteria that form a calcium phosphate shell.

The other factor that leads to stone production is the formation of Randall’s plaques. Calcium oxalate precipitates form in the basement membrane of the thin loops of Henle; these eventually accumulate in the subepithelial space of the renal papillae, leading to a Randall’s plaque and eventually a calculus.
PATHOPHYSIOLOGY
Renal colic occurs in the setting of a fixed or dynamic urinary tract obstruction. Pain associated with urinary tract obstruction results from stretching of the mucosal or submucosal nerve endings of the collecting system or ureteral mucosa by stones and from interstitial edema and distention of the renal capsule.
MAKING THE DIAGNOSIS
The term “renal colic” is a misnomer. Renal colic does not wax and wane like intestinal or biliary colic, but is relatively constant. The pain is of sudden onset and radiates across the abdomen along the course of the ureter; it may be referred to the groin or genital area. Changing position does not relieve the pain. In contrast, patients with acute peritonitis lie still and resist moving.
In patients with renal colic attributable to stone disease, the severity and location of the pain can vary depending on stone size, location and severity of the obstruction, and variations in anatomy and pain threshold. Occasionally, pain may be intermittent as a result of ureteral spasms caused by changes in intraluminal pressure. The character of the pain may vary as the stone passes down the ureter, or it may diminish with the transition from a hyperperistaltic to an aperistaltic ureter.
In addition to pain, patients with acute urinary tract obstruction often present with constitutional symptoms such as anorexia, nausea, vomiting, and abdominal distention. Fever, chills, tachycardia, and hypotension suggest infection.
Investigation-
- Urine R/E
- USG of KUB
- X-ray KUB
- Serum Creatinine
- CBC
- CT Scan (sometimes)
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of renal colic is broad. Flank pain may originate from either renal or nonrenal causes . Causes of blood clots that result in obstruction include glomerulonephritis, hemophilia, sickle cell disease, and tumors. Fungal bezoars (usually Candida or Aspergillus) are common in neonates and immunocompromised hosts. Commonly seen conditions that must be distinguished from renal colic include ectopic pregnancy, aortic aneurysm, and acute intestinal obstruction. One must also be alert for malingerers seeking pain medication or secondary gain.
Treatments : ACKU Facilities
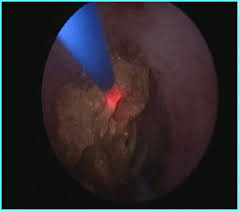
- RETROGRADE INTRARENAL SURGERY (RIRS) : for small renal and upper ureteric stone by Flexible Ureteroscopy and Laser Lithotripsy. ACKU provides world class most sophisticated flexible Ureteroscope with HD Video Camera and 30W Holmium Laser Lithotripsy.
- Ureteroscopy for Ureteric Stone (URS) for mid and lower Ureteric stone by Semirigid Ureteroscopy and Laser Lithotripsy.



ACKU has all caliber Ureteroscope, Even we can do in Children by 4.5 Fr. URS, 6 FR, 7 FR, 8 FR, 9.5 FR Ureteroscope of Storz and Olympus equipped with all accessories by COOK.
After removal of the stone hospital stay is only 6-8 hours.

Quick Links
Contact Centre
- General enquiries
+88 02 9145809
+88 02 9145808
+88 01746 344179 - Request a call back
Can we call you back at a more convenient time - Email us
Send us an email enquiry and we will get back to you.